






J. Clin. Med. 2024, 13(9), 2514; https://doi.org/10.3390/jcm13092514 (registering DOI) - 25 Apr 2024
Abstract
(1) Background: The increasing life expectancy brings an increase in geriatric syndromes, specifically frailty. The literature shows that exercise is a key to preventing, or even reversing, frailty in community-dwelling populations. The main objective is to demonstrate how an intervention based on multicomponent
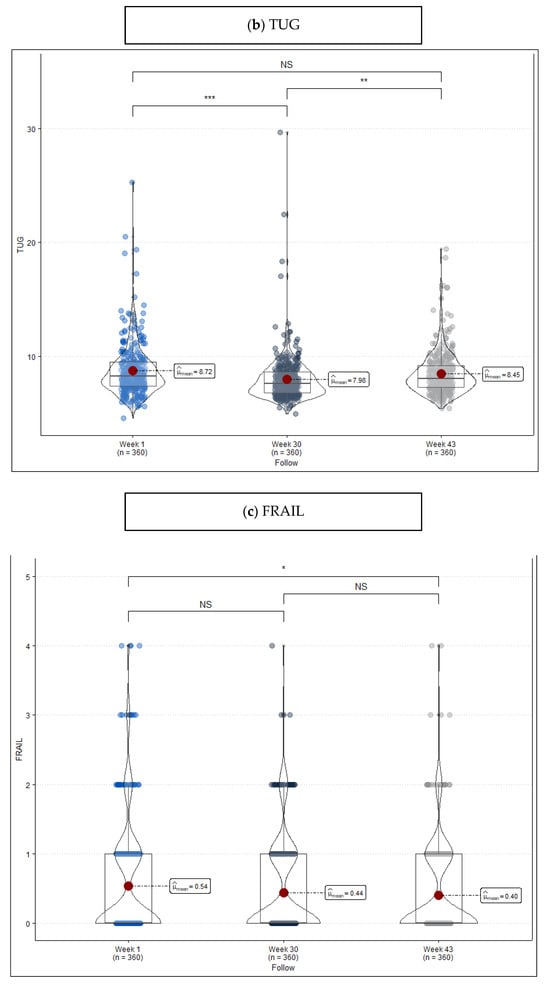
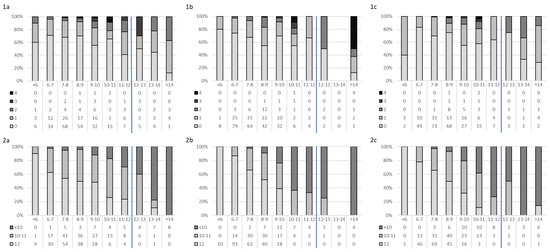
[...] Read more.
(1) Background: The increasing life expectancy brings an increase in geriatric syndromes, specifically frailty. The literature shows that exercise is a key to preventing, or even reversing, frailty in community-dwelling populations. The main objective is to demonstrate how an intervention based on multicomponent exercise produces an improvement in frailty and pre-frailty in a community-dwelling population. (2) Methods: a prospective observational study of a multicomponent exercise program for geriatric revitalization with people aged over 65 holding Barthel Index scores equal to, or beyond, 90. The program was developed over 30 weeks, three times a week, in sessions lasting 45–50 min each. Frailty levels were registered by the Short Physical Performance Battery, FRAIL Questionnaire Screening Tool, and Timed “Up & Go” at the beginning of the program, 30 weeks later (at the end of the program), and following 13 weeks without training; (3) Results: 360 participants completed the program; a greater risk of frailty was found before the program started among older women living in urban areas, with a more elevated fat percentage, more baseline pathologies, and wider baseline medication use. Furthermore, heterogeneous results were observed both in training periods and in periods without physical activity. However, they are consistent over time and show improvement after training. They show a good correlation between TUG and SPPB; (4) Conclusions: A thirty-week multicomponent exercise program improves frailty and pre-frailty status in a community-dwelling population with no functional decline. Nevertheless, a lack of homogeneity is evident among the various tools used for measuring frailty over training periods and inactivity periods.
Full article
(This article belongs to the Special Issue Multidimensional Frailty: The Role of Comprehensive Geriatric Assessment)
►
Show Figures

Figure 1






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}